
15 results
Clinical factors and diagnoses associated with inappropriate urine-culture ordering in primary care
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s1
-
- Article
-
- You have access
- Open access
- Export citation
Identifying nonprescription antibiotic users with screening questions in a primary care setting
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s20-s21
-
- Article
-
- You have access
- Open access
- Export citation
-
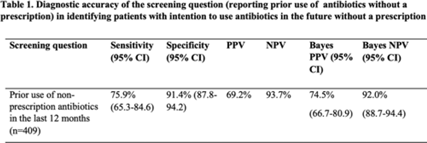
Background: Antibiotic use without a prescription (nonprescription use) leads to antibiotic overuse, with negative consequences for patient and public health. We studied whether screening patients for prior nonprescription antibiotic use in the past 12 months predicted their intentions to use them in the future. Methods: A survey asking respondents about prior and intended nonprescription antibiotic use was performed between January 2020 and June 2021 among patients in waiting rooms of 6 public clinics and 2 private emergency departments in economically and socially diverse urban and suburban areas. Respondents were classified as prior nonprescription users if they reported previously taking oral antibiotics without contacting a doctor, dentist, or nurse. Intended use was defined as answering “yes” or “maybe” to the question, “Would you use antibiotics without contacting a doctor, nurse, or dentist?” We calculated the sensitivity, specificity, and positive and negative predictive value (PPV and NPV) of prior nonprescription antibiotic use in the past 12 months for future intended nonprescription use. Bayes PPV and NPV were also calculated, considering the prevalence of nonprescription antibiotic use (24.8%) in our study. Results: Of the 564 patients surveyed, the median age was 51 years (SD, 19–92), with 72% of patients identifying as female. Most were from the public healthcare system (72.5%). Most respondents identified as Hispanic or Latino(a) (47%) or African American (33%), and 57% received Medicaid or the county financial assistance program. Prior nonprescription use was reported by 246 (43%) of 564 individuals, with 91 (16%) reporting nonprescription use within the previous 12 months. Intention to use nonprescription antibiotics was reported by 140 participants (25%). The sensitivity and specificity of prior nonprescription use in the past 12 months to predict the intention to use nonprescription antibiotics in the future were 75.9% (95% CI, 65.3–84.6) and 91.4% (95% CI, 87.8–94.2), respectively. After the Bayes’ adjustment, the PPV and NPV of prior use to predict future intention were 74.5% (95% CI, 66.7–80.9) and 92.0% (95% CI, 88.7–94.4) (Table 1). Conclusions: These results show that prior nonprescription antibiotic use in the past 12 months predicted the intention to use nonprescription antibiotics in the future (PPV of 75%). As a stewardship effort, we suggest clinicians use a simple question about prior nonprescription antibiotic use in primary-care settings as a screening question for patients at high risk for future nonprescription antibiotic use.
Financial support: HSQR-R 5R01HS026901-04
Disclosure: None

Perspectives on nonprescription antibiotic use among Hispanic patients in the Houston metroplex: A qualitative study
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s20
-
- Article
-
- You have access
- Open access
- Export citation
-
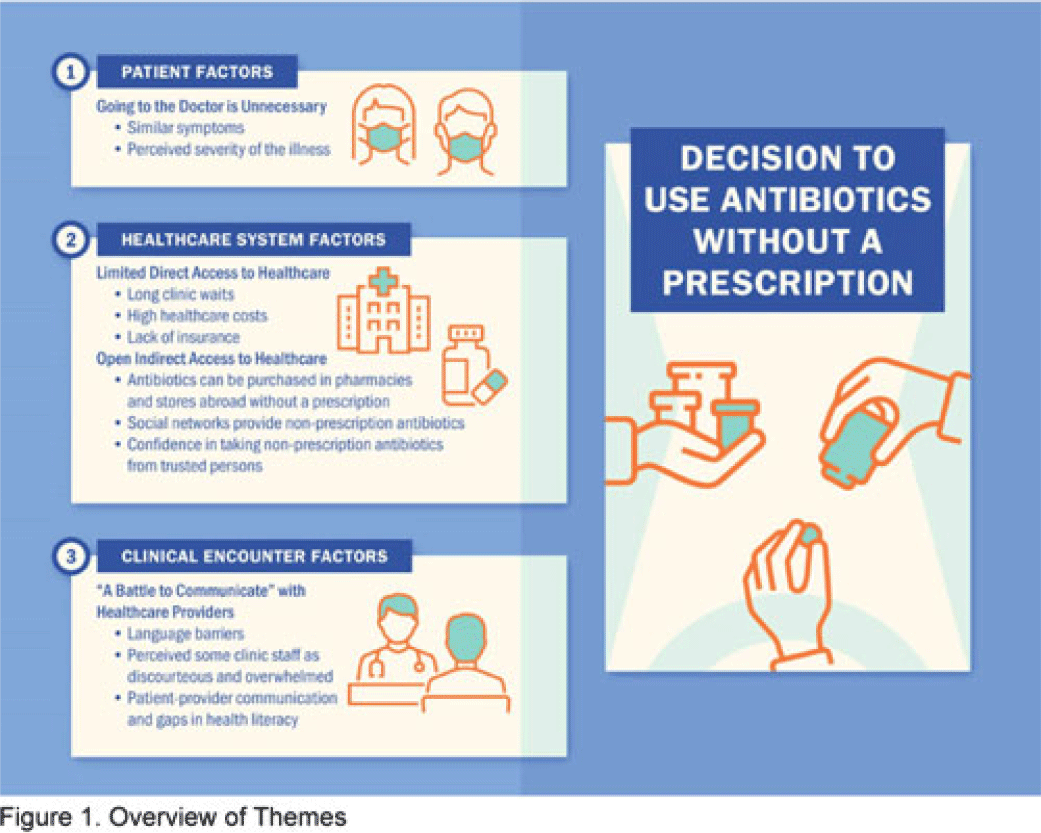
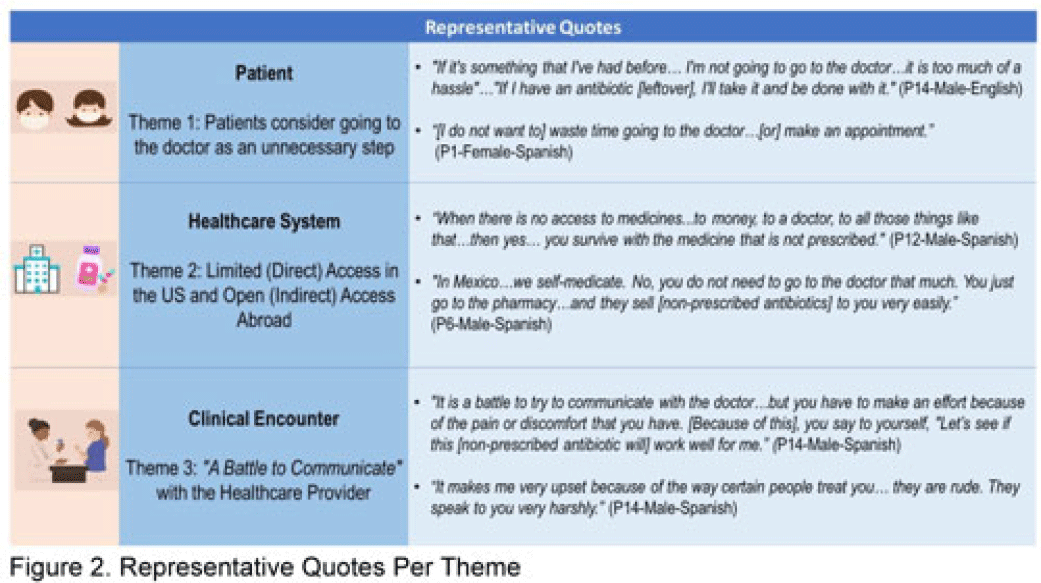
Background: Nonprescription antibiotic use includes taking an antibiotic without medical guidance (eg, leftover antibiotics, antibiotics from friends or relatives, or antibiotics purchased without a prescription). Nonprescription use contributes to antimicrobial resistance, adverse drug reactions, interactions, and superinfections such as Clostridioides difficile colitis. Qualitative studies exploring perspectives regarding nonprescription use among Hispanic patients are lacking. We used the Kilbourne Framework for Advancing Health Disparities Research to identify factors influencing Hispanic patients’ nonprescription use and to organize our findings. Methods: Our study includes Hispanic primary-care clinic patients with different types of health coverage in the Houston metroplex who endorsed nonprescription use in a previous quantitative survey. Semistructured interviews explored the factors promoting nonprescription use in Hispanic adults. Interviews were conducted remotely, in English or Spanish, between May 2020 and October 2021. We used inductive coding and thematic analysis to identify the factors and motives for nonprescription use. Results: Of the 35 Hispanic participants surveyed, 69% were female and between the ages of 27 and 66. All participants had some form of healthcare coverage (eg, Medicare or private insurance, Medicaid, or the county financial assistance program). Participants reported obtaining antibiotics from their own leftover prescriptions and through trusted persons (eg, herbalists, pharmacists, friends/relatives, and others), buying them under the counter in US markets, and purchasing them without a prescription outside the United States. Thematic analysis revealed the factors contributing to nonprescription use (Fig. 1). Themes included beliefs that the ‘doctor visit was unnecessary,’ ‘limited direct access to healthcare’ in the United States (due to limited insurance coverage, high costs of the doctor’s visits and medications, and long clinic wait times), ‘more open indirect access to healthcare’ abroad and under the counter in the United States, and communication difficulties (eg, language barriers with clinicians, perceived staff rudeness, and gaps in health literacy). Figure 2 shows representative quotes across thematic domains. Participants expressed having confidence in medical recommendations from pharmacists and trusted community members in their social networks. Conclusions: Antibiotic stewardship interventions that include pharmacist-driven patient education regarding appropriate antibiotic use may decrease nonprescription antibiotic use in Hispanic communities. Additionally, improving access to care while addressing communication barriers and cultural competency in clinics may improve primary care delivery and reduce potentially unsafe antibiotic use.
Disclosure: None


Quantifying the Implementation and Cost of a Multisite Antibiotic Stewardship Intervention for Asymptomatic Bacteriuria
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 30 June 2023, e115
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Identifying symptoms/illnesses and situations that predispose outpatients to use antibiotics in two healthcare systems – CORRIGENDUM
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue 1 / 2022
- Published online by Cambridge University Press:
- 04 October 2022, e164
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Identifying symptoms/illnesses and situations that predispose outpatients to use antibiotics in two healthcare systems
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, pp. s68-s69
-
- Article
-
- You have access
- Open access
- Export citation
-
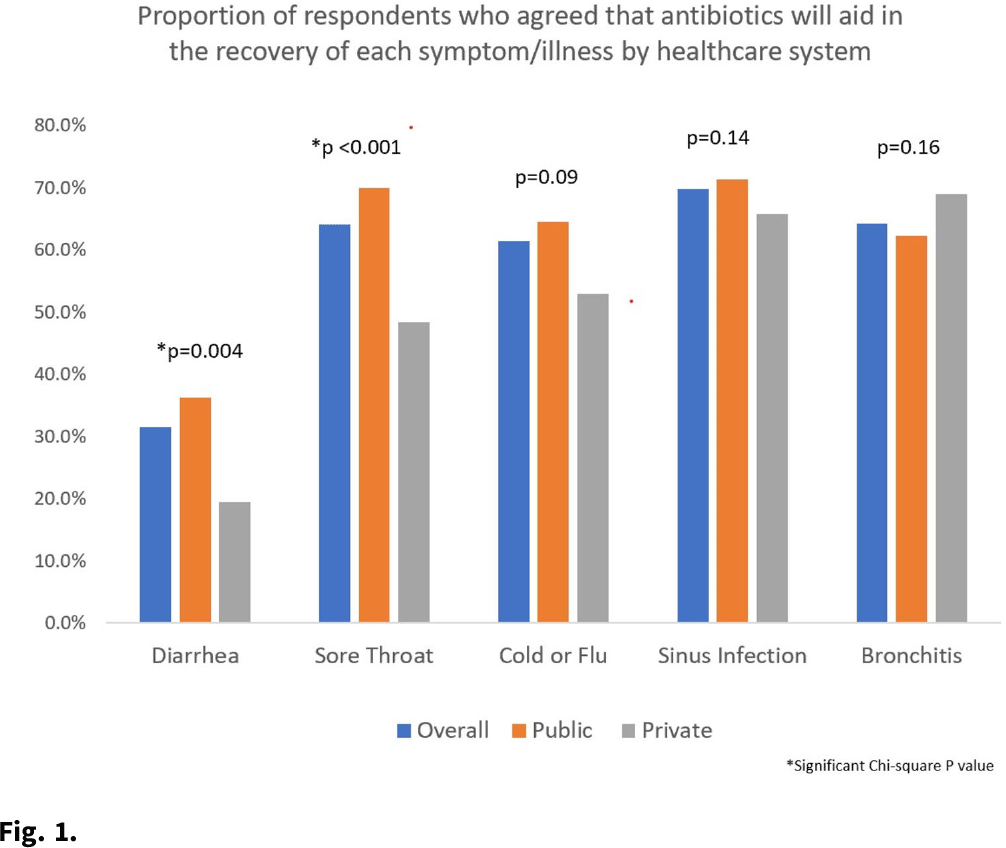
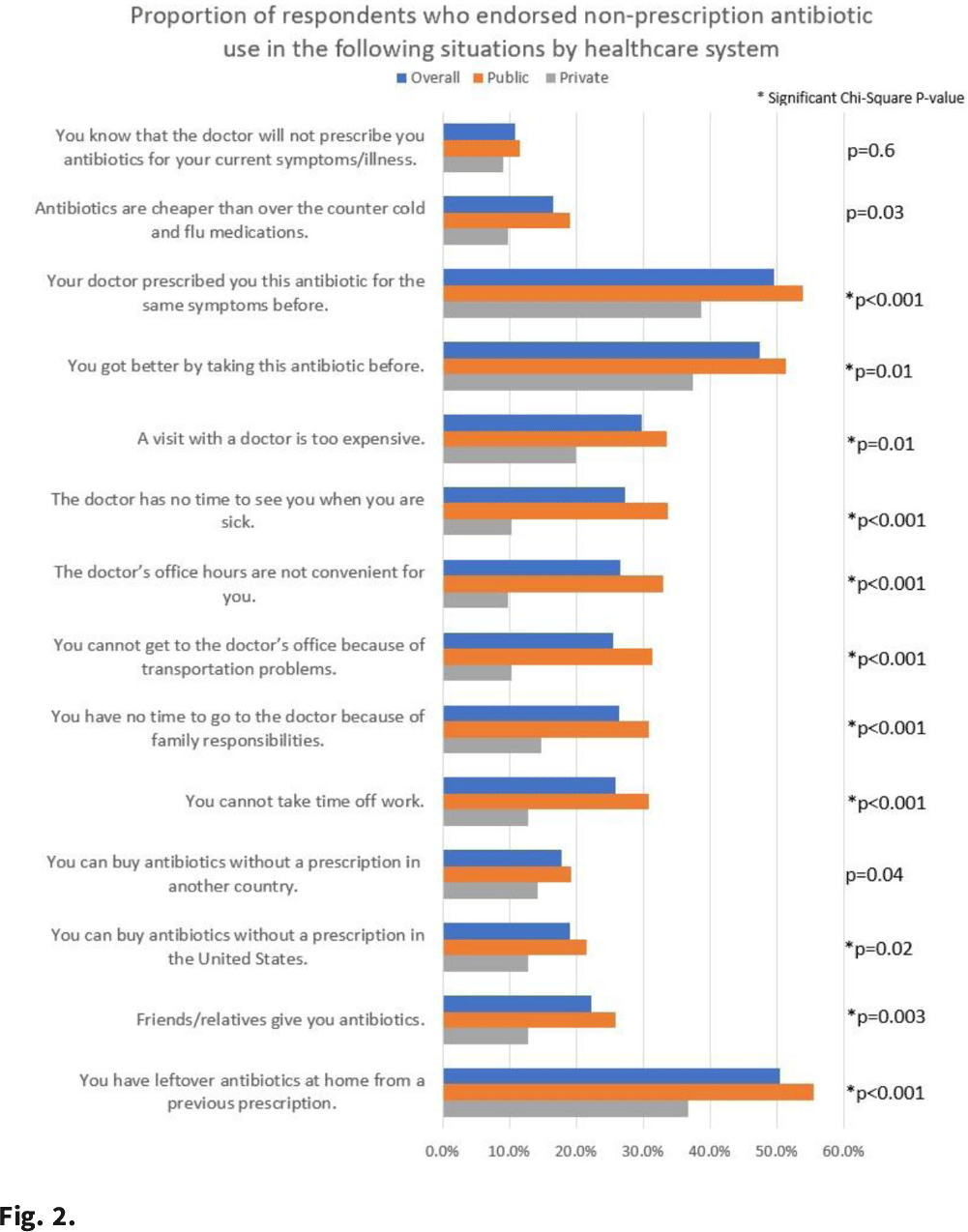
Background: Taking antibiotics outside the guidance of a clinician (nonprescription use) is a potential safety issue and runs counter to antibiotic stewardship efforts. We identified the symptoms and illnesses and situations that may predispose patients to take antibiotics, and we compared these findings between patients attending public primary care clinics and private emergency departments. Methods: A cross-sectional survey was conducted between January 2020 and March 2021 in 6 primary care clinics and 2 emergency departments in the United States. We queried patients about 5 symptoms and illnesses (Fig. 1) and 14 situations (Fig. 2) to investigate whether these would lead the patients to take antibiotics without a prescription. We used the χ2 test to compare the symptoms and illnesses and situations between the respondents from public and private healthcare systems. We set the P value for significance at <.025. Results: In total, the survey had 564 respondents (median age, 49.7 years; range, 19–92), and 72% were female. Most respondents identified as either Hispanic or Latina/Latino (46.6%) or African American or Black (33%), followed by White (15.8%), and other (4.6%). Most respondents had visited public clinics (72%). The most common insurance status for our respondents included Medicaid or county financial assistance program (56.6%), followed by private insurance or Medicare (36.7%) and self-pay (6.7%). In public primary care clinics, only 23% had private insurance or Medicare compared to 72.9% in private emergency departments. Of those surveyed, 69% agreed that antibiotics would improve the recovery from sinus infections, followed by bronchitis (64%), sore throat (64%), cold/flu (61.4%), and diarrhea (31.5%). The proportions of respondents who believed that antibiotics would improve the recovery from diarrhea (36.2% vs 19.4%; P = .004) and sore throat (59.9% vs 48.4%; P < .001) were significantly higher among public versus private outpatient respondents. We did not find significant differences for cold/flu, sinus infection, or bronchitis between these 2 healthcare systems (Fig. 1). In 11 of the 14 situations, patients in public clinics were more likely to report a likelihood of using nonprescription antibiotics than the patients visiting the private emergency rooms (Fig. 2). Conclusions: Future stewardship interventions should be aware of the symptoms and illnesses and situations that may influence outpatients to take nonprescription antibiotics. Addressing modifiable factors (eg, leftover antibiotics, antibiotics given by friends or family, and antibiotics available without a prescription in stores or markets) may also curtail these unsafe practices and reduce antibiotic resistance.
Funding: None
Disclosures: None


Prior cultures predict subsequent susceptibility in patients with recurrent urinary tract infections
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, p. s67
-
- Article
-
- You have access
- Open access
- Export citation
-
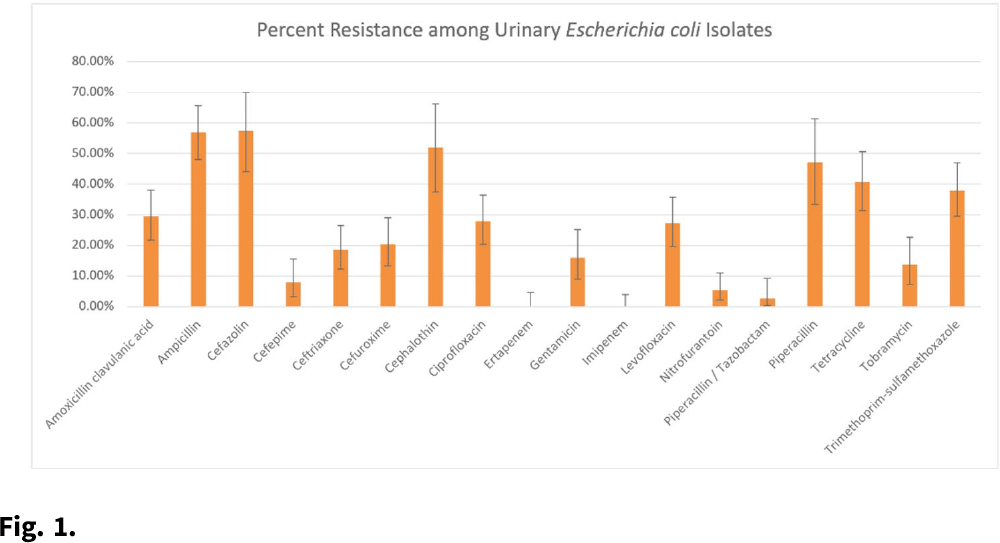
Background: Patients with recurrent urinary tract infections (rUTI) experience frequent exposure to antimicrobial regimens, leaving them at higher risk for developing antibiotic resistance. Little information on the prevalence of antibiotic resistance among patients with rUTI has been published. Although the IDSA recommends using a prior culture to guide empiric treatment, studies have not examined the predictive ability of a prior culture among patients meeting rUTI criteria. We constructed an antibiogram and evaluated test metrics, including sensitivity, specificity, and positive predictive value (PPV) and negative predictive values (NPV) of a prior culture (any organism), on predicting resistance (PPV) or susceptibility (NPV) of a future culture among patients with uncomplicated rUTI in an outpatient setting. Methods: We retrospectively extracted electronic health record data from outpatients aged ≥18 years who had an ICD-10 code for cystitis listed twice in 6 months or thrice in 12 months between November 1, 2016, and December 31, 2018. Patients sought care at either urology or primary care practices within an academic medical center in Houston, Texas. Patients with functional or structural abnormalities of the genitourinary tract, signs or symptoms of pyelonephritis, or pregnancy were excluded. Antibiogram data were reported for uropathogens with ≥30 isolates, and intermediate results were considered resistant. Test metrics and Bayes’ PPV and NPV were calculated using standard formulas. Results: We included 597 visits from 232 unique patients. Most were White (63%) and female (92%), and the cohort had a median age of 58 (IQR, 41–68). Among 310 rUTI episodes with a urine culture, 189 (61%) had at least 1 uropathogen isolated, and Escherichia coli (n = 130, 66%) was most common among all 196 uropathogens. E. coli isolates had >20% resistance to 10 of 18 antibiotics (Fig. 1). E. coli resistance to ciprofloxacin was 27.9%, resistance to nitrofurantoin was 5.5%, and resistance to trimethoprim-sulfamethoxazole was 38.0%. The PPVs for predicting resistance were highest for ceftriaxone (0.86; 95% CI, 0.60–0.96), ciprofloxacin (0.84; 95% CI, 0.63–0.94), and levofloxacin (0.84; 95% CI, 0.63–0.94). NPVs of resistance were highest for gentamicin (0.97; 95% CI, 0.83–1.00), ceftriaxone (0.94; 95% CI, 0.86–0.98), and cefepime (0.94; 95% CI, 0.84–0.98), whereas NPVs for cefuroxime, ciprofloxacin, levofloxacin, and nitrofurantoin were all >0.83. Conclusions: We detected considerable antibiotic resistance among patients with rUTI to commonly prescribed antibiotics. Prior urine culture susceptibility demonstrated moderate-to-high PPVs for predicting future resistance to ceftriaxone and fluoroquinolones as well as high NPVs for several cephalosporins and fluoroquinolones, which could inform empiric prescribing choices.
Funding: This investigator-initiated research study was funded by Rebiotix, a Ferring Company.
Disclosures: None

Analysis of recurrent urinary tract infection management in women seen in outpatient settings reveals opportunities for antibiotic stewardship interventions
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue 1 / 2022
- Published online by Cambridge University Press:
- 17 January 2022, e8
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Analysis of Recurrent Urinary Tract Infection Management in Outpatient Settings Reveals Opportunities for Antibiotic Stewards
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, p. s34
-
- Article
-
- You have access
- Open access
- Export citation
Optimizing Urine Collection Represents an Important Stewardship Opportunity in Primary Care
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, pp. s14-s15
-
- Article
-
- You have access
- Open access
- Export citation
-
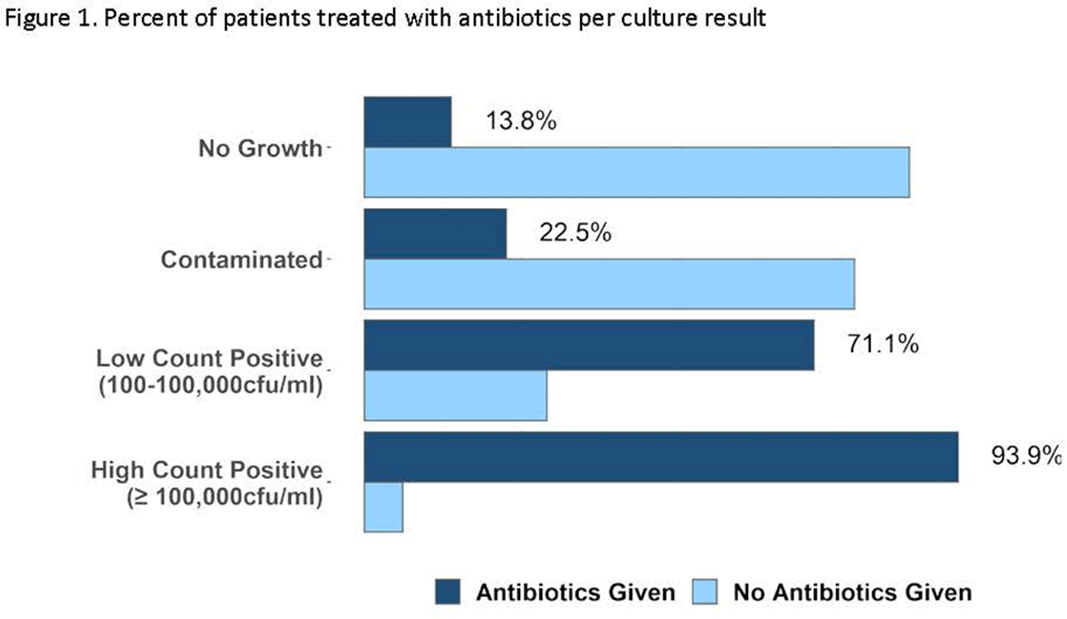
Background: Urine cultures are the most common microbiological tests in the outpatient setting and heavily influence treatment of suspected urinary tract infections (UTIs). Antibiotics for UTI are usually prescribed on an empiric basis in primary care before the urine culture results are available. However, culture results may be needed to confirm a UTI diagnosis and to verify that the correct antibiotic was prescribed. Although urine cultures are considered as the gold standard for diagnosis of UTI, cultures can easily become contaminated during collection. We determined the prevalence, predictors, and antibiotic use associated with contaminated urine cultures in 2 adult safety net primary care clinics. Methods: We conducted a retrospective chart review of visits with provider-suspected UTI in which a urine culture was ordered (November 2018–March 2020). Patient demographics, culture results, and prescription orders were captured for each visit. Culture results were defined as no culture growth, contaminated (ie, mixed flora, non-uropathogens, or ≥3 bacteria isolated on culture), low-count positive (growth between 100 and 100,000 CFU/mL), and high-count positive (>100,000 CFU/mL). A multivariable multinomial logistic regression model was used to identify factors associated with contaminated culture results. Results: There were 1,265 visits with urine cultures: 264 (20.9%) had no growth, 694 (54.9%) were contaminated, 159 (12.6%) were low counts, and 148 (11.7%) were high counts. Encounter-level factors are presented in Table 1. Female gender (adjusted odds ratio [aOR], 15.8; 95% confidence interval [CI], 10.21–23.46; P < .001), pregnancy (aOR, 13.98; 95% CI, 7.93–4.67; P < .001), and obesity (aOR, 1.9; 95% CI 1.31–2.77; P < .001) were independently associated with contaminated cultures. Of 264 patients whose urine cultures showed no growth, 36 (14%) were prescribed an antibiotic. Of 694 patients with contaminated cultures, 153 (22%) were prescribed an antibiotic (Figure 1). Conclusions: More than half of urine cultures were contaminated, and 1 in 5 patients were treated with antibiotics. Reduction of contamination should improve patient care by providing a more accurate record of the organism in the urine (if any) and its susceptibilities, which are relevant to managing future episodes of UTI in that patient. Optimizing urine collection represents a diagnostic stewardship opportunity in primary care.
Funding: This study was supported by the National Institute of Allergy and Infectious Diseases of the National Institutes of Health (grant no. UM1AI104681). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Disclosures: None
Table 1. 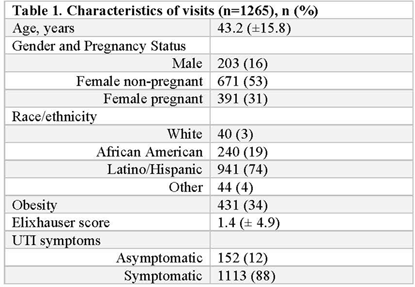
Figure 1.


Organizational Readiness to Change Assessment Highlights Differential Readiness for Antibiotic Stewardship
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s492-s493
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
A Conceptual Framework for Understanding How and Why People Take Antibiotics Without a Prescription
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, p. s93
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Creating an Outpatient-Specific Antibiogram to Guide Treatment for Urinary Tract Infections
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s182-s183
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Effectiveness of Stewardship Intervention for Urinary Tract Infections in Primary Care: A Difference in Differences Study
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s515-s516
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Teamwork and safety climate affect antimicrobial stewardship for asymptomatic bacteriuria
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 40 / Issue 9 / September 2019
- Published online by Cambridge University Press:
- 24 July 2019, pp. 963-967
- Print publication:
- September 2019
-
- Article
- Export citation
